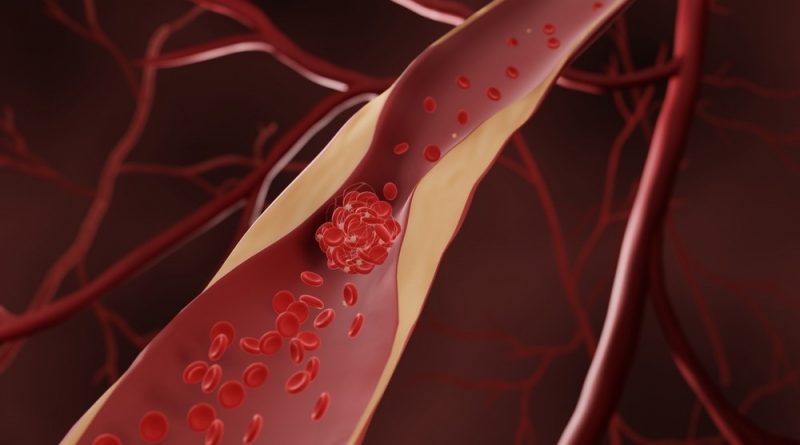
The relationship between intestinal microbiome dysbiosis and atherosclerosis
In a recent review published in the International Journal of Molecular Sciences, researchers in Canada investigate the impact of intestinal microbiota dysbiosis on atherosclerotic cardiovascular disease (ASCVD) incidence.
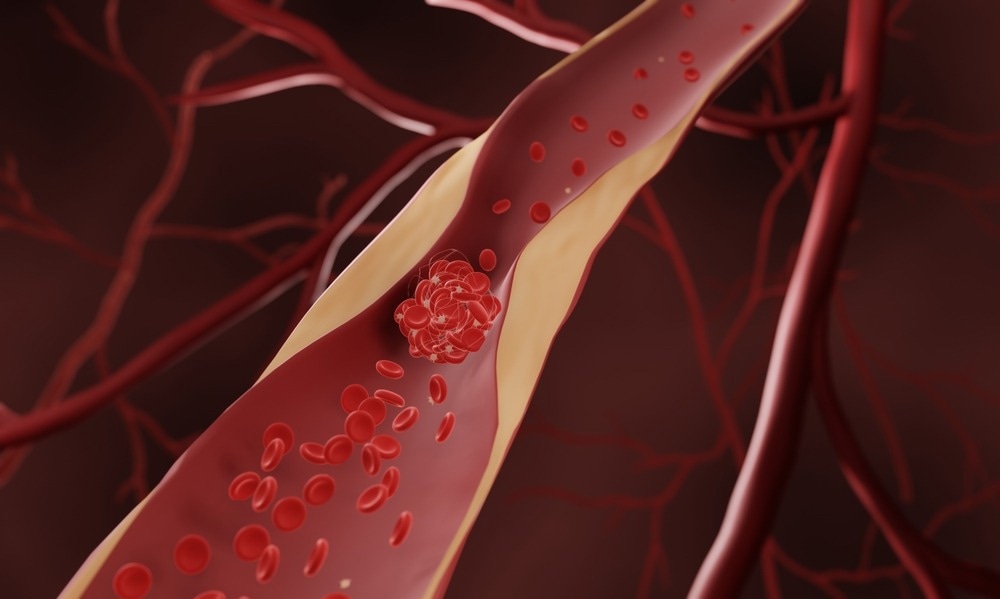
Study: Role of the Gut Microbiome in the Development of Atherosclerotic Cardiovascular Disease. Image Credit: ART-ur / Shutterstock.com
Background
ASCVD is a leading cause of mortality across the globe. A detailed understanding of the association between the gut microbiome and atherosclerosis development is needed to develop preventive and therapeutic strategies, as well as manage key factors that increase the risk of CVD, including diabetes, hypertension, smoking, sedentary lifestyle, and dyslipidemia.
Previous studies have reported that the intestinal microbiota is critically involved in atherosclerosis development. Essential intestinal metabolites, such as trimethylamine N-oxide (TMAO), lipopolysaccharides (LPS), short-chain fatty acids (SCFAs), and secondary-type bile acids are reportedly related to ischemic heart disease severity.
Metabolic pathways of intestinal dysbiosis leading to atherosclerosis
Increased dietary intake of phenylalanine, betaine, L-carnitine, and choline results in increased trimethylamine (TMA) secretion from the gut and TMAO from the liver. This reduces reverse cholesterol transport (RCT) and increases foam cell formation in cholesterol plaques, platelet reactivity, and endothelial dysfunction.
Reduced endothelial progenitor cell (EPC) production is associated with the nucleotide-binding oligomerization domain-like receptor family pyrin domain-containing 3 (NLRP3) inflammasome activation, which increases reactive oxygen species (ROS) levels in mitochondrial pathways.
Elevated secondary-type bile acid secretion occurs in the gut by deconjugation of chenodeoxycholic acid and cholic acid. Secondary-type bile acid molecules enable fat-soluble vitamin and lipid absorption, as well as activate the Takeda G protein-coupled receptor 5 (TGR-5) and farnesoid X receptor (FXR). These receptors modulate cholesterol and glucose metabolism, as well as activate the nuclear factor kappa B (NF-κB) pathway, thereby increasing tumor necrosis factor-alpha (TNF-α), interleukin 1 (IL-1), IL-6, and IL-8 levels.
TGR-5 levels increase glucagon-like peptide 1 (GLP-1) expression, thus improving glucose tolerance. NF-κB pathway activity is enhanced by LPS, which are bacterial endotoxins that are identified by innate immunological pathways through toll-like receptor- 4 (TLR-4), which is a pattern-recognition receptor (PRR).
Comparatively, SCFAs such as acetate, propionate, and butyrate prevent atherosclerosis and are generated from the digestion of complex carbohydrates by intestinal bacteria such as Faecalibacterium prausnitzii, Roseburia intestinalis, and Anaerostipes butyraticus. SCFAs inhibit the NF-κB pathway through enhanced production of regulatory T lymphocytes (Treg) and histone deacetylase (HDAC) suppression and increased gut barrier stability.
Antibodies eBook
Lipopolysaccharides are also recognized by receptor proteins, such as the lipopolysaccharide-binding protein (LBP), cluster of differentiation-14 (CD-14), and myeloid differentiation protein-2 (MD-2).
The receptors, which are largely expressed on macrophage cells, activate and subsequently increase the expression of protein kinase molecules, including myeloid differentiation factor- 88 (MyD88) and IL-1 receptor-associated kinase (IRAK-1).
Phenylacetic acid released from the gut leads to increased expression of phenylacetylglutamine (PAGln) from glutamine and platelet activation. PAGln enhances platelet responsiveness, with a resultant increase in the thrombosis potential that causes ASCVDs.
Furthermore, PAGln transmits cellular events through G-protein coupled receptors such as the α-2A, 2B, and beta-2 (β2) adrenergic receptors. PAGln also accelerates thrombus production and vessel occlusion rates.
Diet and atherosclerosis
A low-fiber diet is linked to lower SCFA concentration in the blood, especially that of butyrate. This can aggravate dysbiosis and inflammation through the leaking of bacterial-origin toxins such as LPS. This inflammation can result in hypertension, diabetes, atherosclerosis, acute coronary syndrome, or myocardial infarction.
LPS induces ROS generation by nicotinamide adenine dinucleotide phosphate (NADPH) oxidase activation, thereby increasing the expression of IL-6, IL-8, and TNF-α. Butyrate increases plaque stability by reducing nitric oxide (NO) and ROS release from macrophages and lowers the production of inflammatory molecules, such as matrix metalloproteinase-2 (MMP-2), vascular cell adhesion molecule-1 (VCAM-1), and chemotaxis protein-1.
A modern westernized diet high in red meat, fish, and eggs releases choline and L-carnitine, which susbequently increases the bacterial generation of TMA. TMA undergoes oxidation to form TMAO in hepatic tissues through flavin-containing monooxygenase 3 (FMO3) activity.
Hypertensive patients have less microbial variety and richness, with reduced Lactobacillus counts and elevated counts of Klebsiella and Prevotella as compared to healthy individuals. This dysbiosis results in inflammation.
SCFAs can lower blood pressure due to their anti-inflammatory and vasorelaxant effects, whereas TMAO causes hypertension due to its prothrombotic, proatherogenic, and angiotensin-II activity-prolonging effects.
TMAO also stiffens the carotid arteries and aorta, reduces high-density lipoprotein-cholesterol (HDL-C) levels, increases cholesterol accumulation in the cells, and enhances the risks of obesity, dyslipidemia, and type 2 diabetes complications. Furthermore, TMAO increases the expression of macrophage receptors, CD-36, and scavenger receptor-A (SR-A), all of which are linked to atherosclerosis. TMAO induces vascular inflammation by increasing leukocyte recruitment to endothelial cells through G protein-coupled receptor (GPCR) activity and enhanced mitogen-activated protein kinase (MAPK) activity.
Conclusions
The current study elucidates the impact of intestinal microbial dysbiosis on atherosclerosis development. These findings indicate that secondary bile acids and SCFAs protect against dyslipidemia, whereas other metabolites, such as TMAO and LPS, increase cholesterol levels.
- Al Samarraie, A., Pichette, M., & Rousseau, G. (2023). Role of the Gut Microbiome in the Development of Atherosclerotic Cardiovascular Disease. International Journal of Molecular Science 24. doi:10.3390/ ijms24065420
Posted in: Medical Science News | Medical Research News | Medical Condition News | Disease/Infection News
Tags: Acute Coronary Syndrome, Adenine, Angiotensin, Anti-Inflammatory, Aorta, Atherosclerosis, Bacteria, Bile, Blood, Blood Pressure, Cardiovascular Disease, Cell, Cell Adhesion, Cholesterol, Diabetes, Diet, Digestion, Dysbiosis, Dyslipidemia, Fatty Acids, Fish, GLP-1, Glucagon, Glucose, Glucose Metabolism, Glutamine, GPCR, G-Protein, Heart, Heart Disease, Inflammasome, Inflammation, Interleukin, Ischemic Heart Disease, Kinase, Lactobacillus, Leukocyte, Lipoprotein, Liver, Macrophage, Meat, Metabolism, Metabolites, Microbiome, Molecule, Mortality, Myocardial Infarction, Necrosis, Nitric Oxide, Nucleotide, Obesity, Oxygen, Phenylalanine, Platelet, Protein, Receptor, Short-Chain Fatty Acids, Smoking, Syndrome, Thrombosis, Thrombus, Toxins, Tumor, Tumor Necrosis Factor, Type 2 Diabetes, Vascular

Written by
Pooja Toshniwal Paharia
Dr. based clinical-radiological diagnosis and management of oral lesions and conditions and associated maxillofacial disorders.
Source: Read Full Article