
Effects of acute and chronic graft-versus-myelodysplastic syndrome on outcomes following cell transplantation
Myelodysplastic syndrome (MDS) is a bone marrow failure disorder characterized by intractable cytopenia and dysplastic hematological changes. MDS has a varied clinical course, with some patients remaining asymptomatic with mild cytopenia for a long time, while others show progressive leukemia a short time after the diagnosis. Allogeneic hematopoietic cell transplantation is considered the only curative treatment.
A research group led by Assistant Professor Takaaki Konuma in the Department of Hematology/Oncology, the Hospital of the Institute of Medical Science, the University of Tokyo (IMSUT Hospital) has demonstrated a graft-versus-tumor (GVT) effect of a previously unknown/novel allogeneic hematopoietic cell transplantation in MDS patients. In addition, they succeeded in identifying a category of patients for whom the GVT effect was identified. These results used data from 3119 MDS patients aged 16 to 70 who are registered at the Japanese Data Center for Hematopoietic Cell Transplantation (JDCHCT).
These results were published online in Clinical Cancer Research, a journal of the American Association for Cancer Research on September 7.
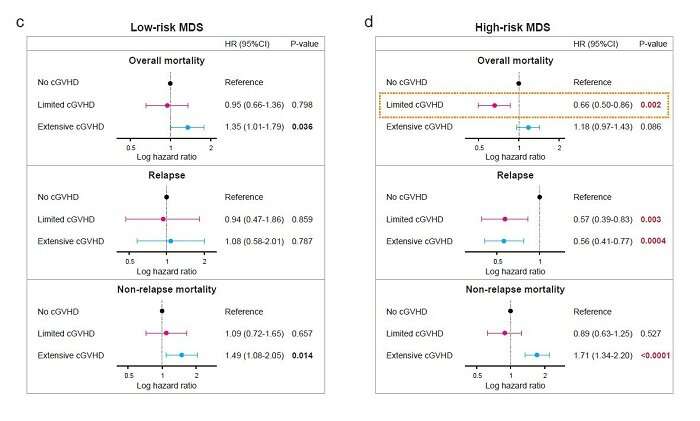
Graft-versus-tumor effect associated with limited chronic GVHD alone improved survival in high-risk MDS
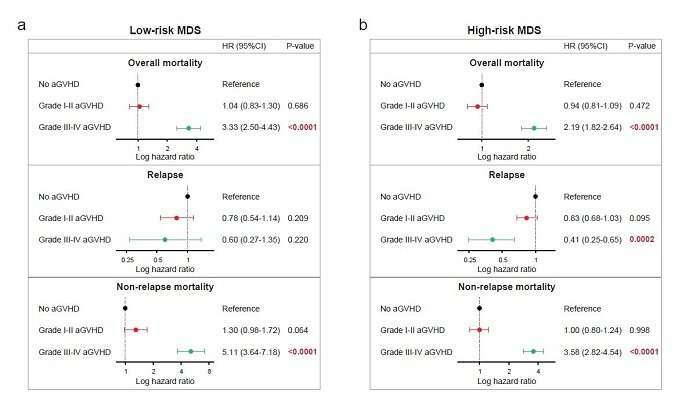
According to Assistant Professor Konuma, the research group retrospectively evaluated the impact of acute and chronic graft-versus-host disease (GVHD) on transplant outcomes for a large cohort of adult patients with a low-risk (n = 1193) or high-risk (n = 1926) of myelodysplastic syndrome (MDS).
Their study demonstrated that for patients with a low-risk of MDS, acute and chronic GVHD at any grade or severity did not improve overall mortality, relapse, or non-relapse mortality (NRM). For patients with a high-risk of MDS, the favorable effect of limited chronic GVHD on disease relapse was associated with a decrease in overall mortality; however, the favorable effects of grade III-IV acute GVHD, or extensive chronic GVHD on disease relapse were offset by increased NRM.
Source: Read Full Article