cialis daily price uk

New results from a study led by USC researchers at Children’s Hospital Los Angeles show that a sensory adapted dental clinic environment creates less distressing oral care experiences for autistic children. The open-access article is available today in JAMA Network Open.
“We’ve shown that the combination of curated visual, auditory and tactile adaptations—all of which are easily implemented, relatively inexpensive and don’t require training to safely use—led to statistically significant decreases in autistic children’s behavioral and physiological distress during dental cleanings,” said lead author Leah Stein Duker, assistant professor at the USC Chan Division of Occupational Science and Occupational Therapy.
Compared to typically developing peers, autistic children experience greater oral health care challenges, which are often associated with heightened responses to sensory input. The dentist’s office is filled with potentially overwhelming stimuli such as bright fluorescent lighting, ranitidine tablets india whirring electric hand tools and reclining chairs. Stein Duker and the Sensory Adapted Dental Environments (SADE) research team, including colleagues from the Ostrow School of Dentistry of USC, are identifying and testing innovative approaches that can help alleviate those challenges in order to increase access and efficacy of oral care.
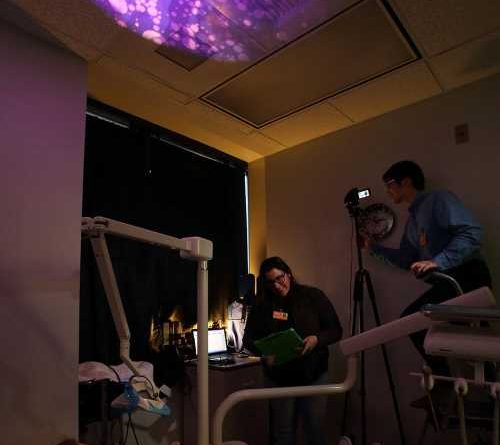
In this study, autistic children received cleanings in both a standard clinic environment and an adapted one. In the adapted setting, the dentist wore a surgical loupe with attached lamp, blackout curtains were hung over the windows and a slow-motion visual effect was projected onto the ceiling (children could choose between a “Finding Nemo” underwater scene or lava lamp-style abstract colors). A portable speaker played calming nature sounds and quiet piano music. A traditional lead X-ray bib placed on the child’s chest and a “butterfly” wrap secured around the dental chair provided deep pressure hugging sensation from shoulder to ankle, which has been shown to calm the nervous system.
Electrodes placed on the child’s fingers measured electrodermal activity, a physiological correlate of sympathetic nervous system activation akin to the fight-or-flight response. The researchers also observed the frequency and duration of distressed behaviors exhibited by the child during the cleaning, such as jerking away from the dentist, clamping down with the jaw, intentionally trying to bite the dentist or keep tools out of the mouth, crying and screaming.
The researchers did not find any differences in the quality of care provided in the adapted environment, compared to the regular environment. They also did not find any significant differences in the amount of time required to get the child seated and ready for the cleaning, demonstrating that adaptations do not create logistical hurdles.
“So many interventions try to change the person” Stein Duker said. “Instead, this intervention sees children for who they are—it does not try to fix or change them—focusing the intervention to modify problematic environmental factors as a way to empower the child and family to engage successfully in occupation.”

Adaptations can make all the difference
This publication is the latest from the SADE research project, led by Principal Investigator Professor Sharon Cermak, which dates back to 2011. Since then, the SADE intervention has been replicated in pilot studies with a number of different populations in several countries. However, Stein Duker said, this study is the first with a large enough sample size to attain full statistical power.
“Because it’s a fully-powered study, we were able to identify some other very exciting findings,” Stein Duker said. “For example, our data showed that children’s physiological stress dropped as soon as they entered the adapted dental cleaning room before the actual cleaning even began, and that level of physiological stress predicted behavioral distress during the cleaning.”
The researchers also identified factors predicting the intervention’s success for any given participant: younger age and lower IQ and/or lower expressive communication level were each associated with a proportionally greater reduction in participants’ stress.
“My daughter cannot even hear the word ‘dentist,'” said one participant’s parent. “But after being in the [SADE] room for a bit, she was able to have her teeth looked at for the first time in over a year.”
In addition to oral care disparities experienced specifically by autistic children, the study may also help close an ethnic disparity gap, as 72 percent of parents of the children enrolled self-identified as Hispanic. (Note: the term “Hispanic” is used in the US to refer to people who identify as Hispanic, Latino, Chicano, Latinx, Latine, etc., which appears to be a preferred pan-ethnic term among those who expressed a preference). Data has shown that Hispanic children in the US have oral health disparities: 52 percent of Hispanic youth ages 2-19 years have dental caries (cavities), which is the highest population prevalence compared to non-Hispanic Black (44 percent), Asian (43 percent) and White (39 percent) youth. Bilingual members of the SADE research team ensured fidelity with Spanish-speaking participants and families.
Stein Duker and her Tailored Environmental Modifications lab will next study the effectiveness of a modified SADE for typically developing children with dental fear and anxiety, a major challenge in pediatric dentistry experienced by approximately 20 percent of all US children. In the near future, she is also planning to collect preliminary data studying adolescents and adults with intellectual developmental disabilities and/or autism, populations she gets frequently asked about at dental conferences and research meetings.
“Regardless of population, my advice to dental professionals and parents alike is to work together to find ways to improve the overall clinic experience,” Stein Duker says. “There are weighted X-ray bibs in every single dental office that may help calm the child; they can wear sunglasses; they can wear a beanie hat covering the ears to muffle noises—all of these are completely free and easy adaptations that have the potential to improve the clinic experience for those with sensory sensitivities, without negatively impacting dentists’ ability to provide care.”
More information:
Leah I. Stein Duker et al, Sensory Adaptations to Improve Physiological and Behavioral Distress During Dental Visits in Autistic Children, JAMA Network Open (2023). DOI: 10.1001/jamanetworkopen.2023.16346
Journal information:
JAMA Network Open
Source: Read Full Article